

A Case of Stent and Catheter Aspiration Thrombectomy for Cerebral Venous Sinus Thrombosis
Date:2025-04-23Category:Case ReportsViews:1380
Zenith devices used in this case:

Patient Information
- Male, 41 years old
- Headache for 10 days, episodic seizures for 8 days
- Conscious, fluent speech
- Normal strength in the left limbs, right extremity muscle strength at grade 4, no meningeal signs
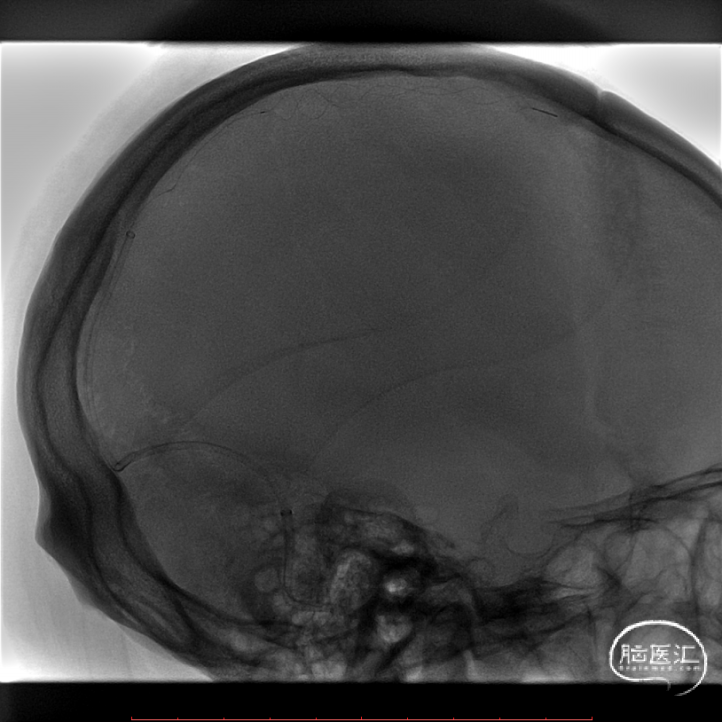
Preoperative Angiography
Preoperative brain MRI revealed a hemorrhagic infarction in the left frontoparietal lobe accompanied by cerebral edema.

MRV demonstrated extensive thrombosis in the superior sagittal sinus, with poor visualization of the right transverse and sigmoid sinuses.

Devices
- 5F 125cm Angiographic Catheter
- Hydrophilic Wire
- 6F 90cm Zenith Long Sheath
- 6F 125cm Zenith Aspiration Catheter
- 014”200cm Microguide Wire
- 6mm x 35mm Stent Retriever
- Zenith Aspiration Pump
Procedure
The procedure began with right femoral artery puncture, followed by the insertion of a 6F vascular sheath. A 5F single-curve diagnostic catheter, guided by a hydrophilic wire, was used for cerebral angiography. Venous phase imaging showed interrupted and narrowed filling of the superior sagittal sinus, cortical venous congestion, and poor visualization of the right transverse and sigmoid sinuses.

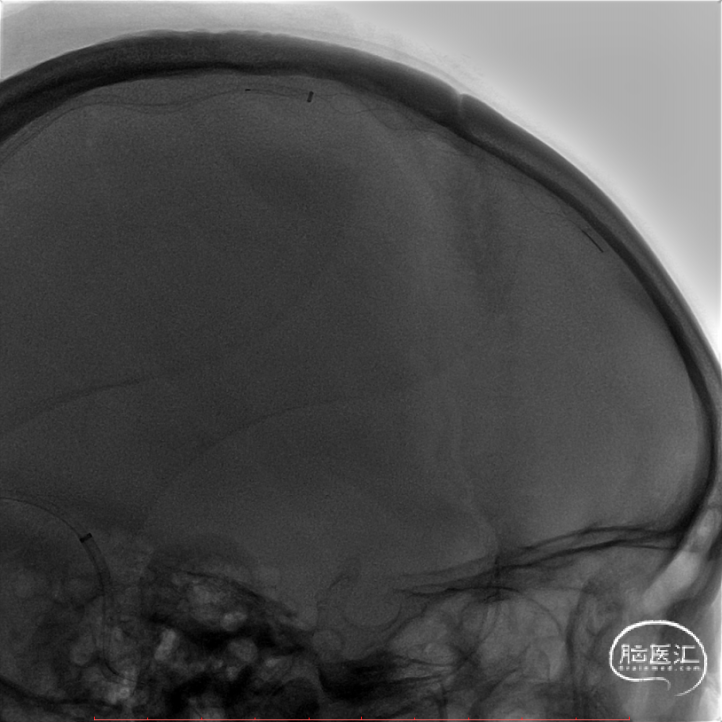
The right femoral vein access was established with an 8F vascular sheath. Under the guidance of a 0.035" wire and a 5F 125cm multi-purpose catheter, a 6F 90cm Zenith Long Sheath was advanced into the right jugular bulb. A 6F 125cm Zenith Aspiration Catheter was then navigated through the right sigmoid sinus into the superior sagittal sinus, with the long sheath following into the right sigmoid sinus to provide additional support. A 0.014" microguide wire and a 0.021" Zenith Microcatheter were advanced into the anterior segment of the superior sagittal sinus, where venography confirmed the presence of extensive thrombosis.

A 6mm × 35mm stent retriever was deployed in the superior sagittal sinus.
The aspiration catheter was connected to a vacuum pump, and under continuous aspiration, it was carefully maneuvered back and forth along the stent wire to retrieve thrombi.
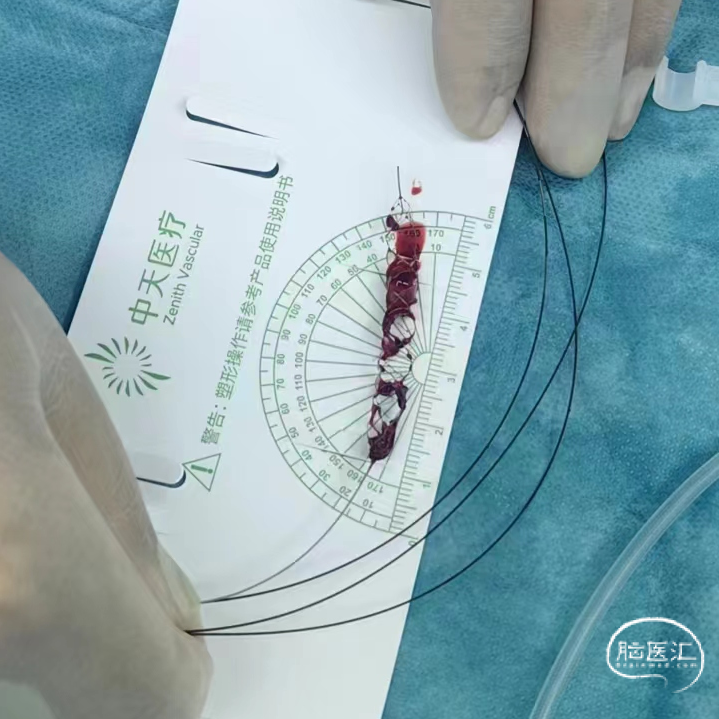
A substantial amount of thrombus was observed within the stent and the aspiration reservoir.

Post-thrombectomy angiography showed improved filling of the mid and lower superior sagittal sinus, the confluence of sinuses, and the right transverse sinus, but persistent poor visualization of the anterior segment of the superior sagittal sinus.

The microcatheter was advanced further into the anterior segment of the superior sagittal sinus, where a Syphonet stent retriever was deployed. The aspiration catheter was then introduced to perform additional thrombectomy in this segment.
Under continuous vacuum aspiration, the stent retriever was withdrawn, successfully retrieving more thrombus. Angiography through the aspiration catheter showed improved perfusion in the anterior superior sagittal sinus.

Follow-up angiography demonstrated enhanced visualization of the superior sagittal sinus, significant reduction in cortical venous congestion, and a remaining filling defect at the confluence of sinuses.

For the final step, a stent retriever was deployed at the confluence of sinuses. The aspiration catheter was gradually retracted under continuous aspiration, extending down to the jugular bulb. Final angiography confirmed significant improvement in flow through the superior sagittal sinus, confluence, right transverse sinus, and sigmoid sinus.

Postoperative Examination
- Headache significantly relieved,no further episodes of consciousness loss or seizures
- Neurological examination: Conscious, fluent speech, extremity strength unchanged from pre-op, no meningeal signs
Surgeon Information
Guiping Wang, Shanghai Blue Cross Brain Hospital