

A Case of Endovascular Recanalization and Thrombectomy for Right ICA Occlusion
Date:2026-04-12Category:Case ReportsViews:261
Zenith device used in this case:

Patient Information
- Male, 67 years old
- Slurred speech and left limb weakness for 1 hour.
- Muscle strength: Left limbs – Grade 0, Right limbs – Normal
- NIHSS score: 15 points
- mRS score: 4 points
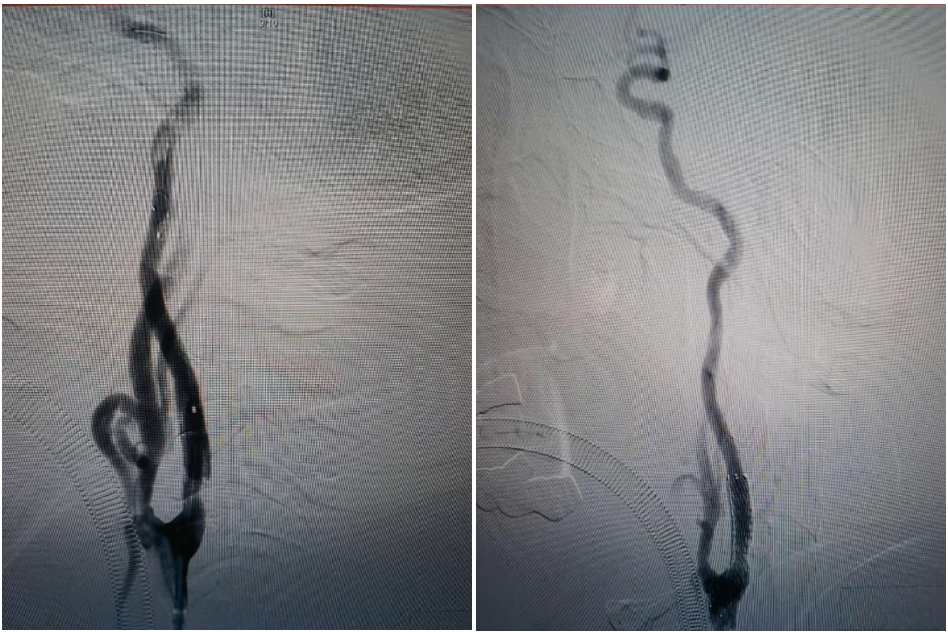
Preoperative Angiography
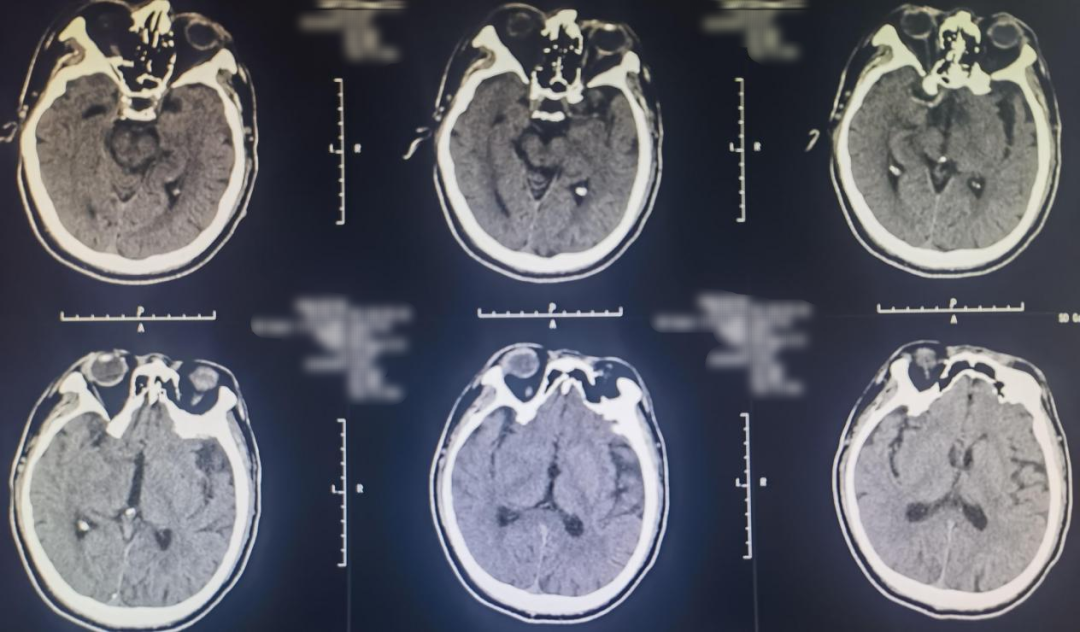
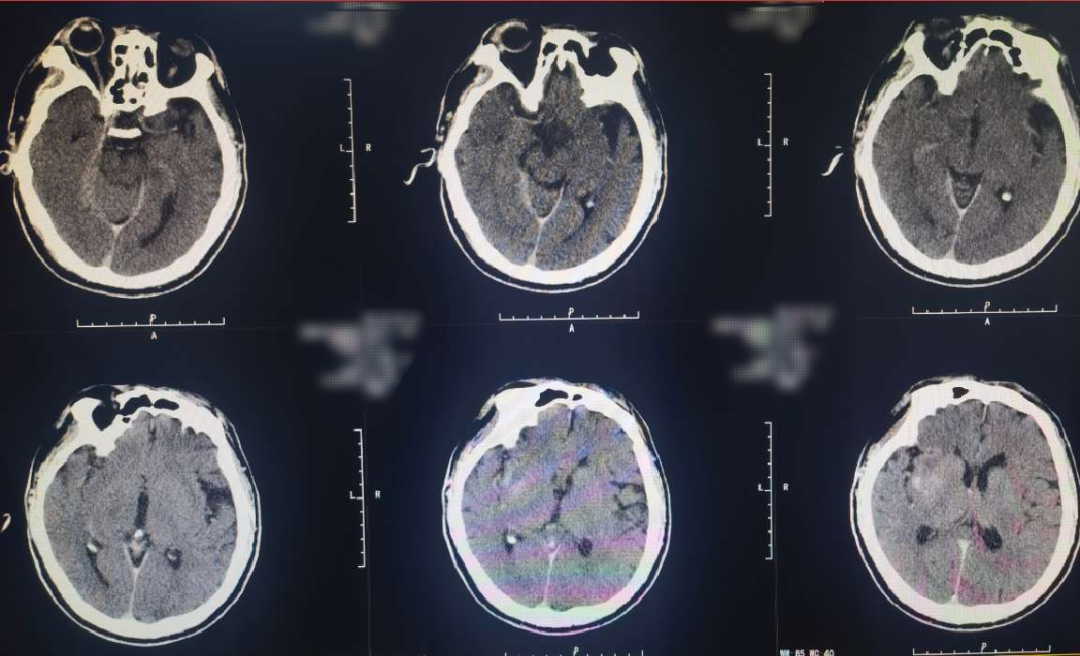
Cranial CT revealed a hyperdense sign in the right middle cerebral artery.
Preoperative MRI:
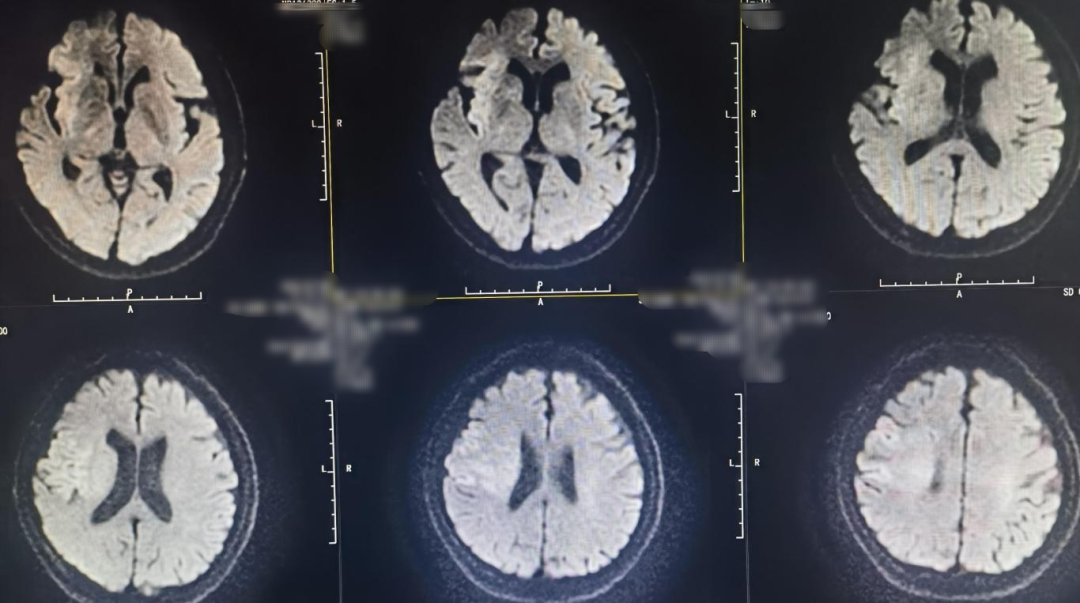

Right internal carotid angiography showed occlusion of the right ICA, with no collateral circulation in the right ACA or right MCA, and no compensatory blood flow in the surrounding area.

Devices
- MPA 8F Guiding Catheter
- 0.014in*200cm、0.014in*300cm Microwire
- 2.5mm*20mm、4.0mm*30mm Balloon
- Microcatheter
- 6F Zenith Aspiration Catheter
- 5.0mm Embolic Protection Device
- 7*40mm Carotid Stent
Procedure
A microguidewire and microcatheter were carefully advanced through the occluded origin of the right ICA. Contrast injection through the microcatheter confirmed its position in the true lumen of the ICA. The microcatheter was exchanged for a long guidewire and withdrawn. A 2.5 mm balloon was used for pre-dilation at the occluded segment of the right ICA origin, followed by advancement of an 8F guiding catheter. A Zenith Aspiration Catheter was introduced coaxially and advanced along the ICA. Aspiration yielded a large amount of thrombus.

Post-aspiration angiography demonstrated good visualization of the right MCA and ACA.

To further manage severe stenosis at the origin of the right ICA, the aspiration catheter was withdrawn. A distal protection device was deployed through the 8F guiding catheter, which was then retracted to the common carotid artery. A peripheral balloon dilation catheter was advanced along the protection guidewire to the stenotic segment for angioplasty. After balloon dilation, a Wallstent was delivered along the protection guidewire and precisely deployed at the stenotic site. Post-deployment angiography showed good stent apposition, with a residual stenosis rate of approximately 20%. Antegrade blood flow and intracranial perfusion improved, achieving TICI grade 3 flow.
Postoperative Angiography
The right MCA, ACA, and their branch arteries were well visualized, with antegrade flow of TICI grade 3 and no signs of acute vascular occlusion.

Immediate postoperative CT showed no secondary hemorrhage but mild contrast retention.
At 6 hours post-operation, the patient was somnolent, with left limb muscle strength of grade 2 and normal strength on the right. NIHSS score: 11.
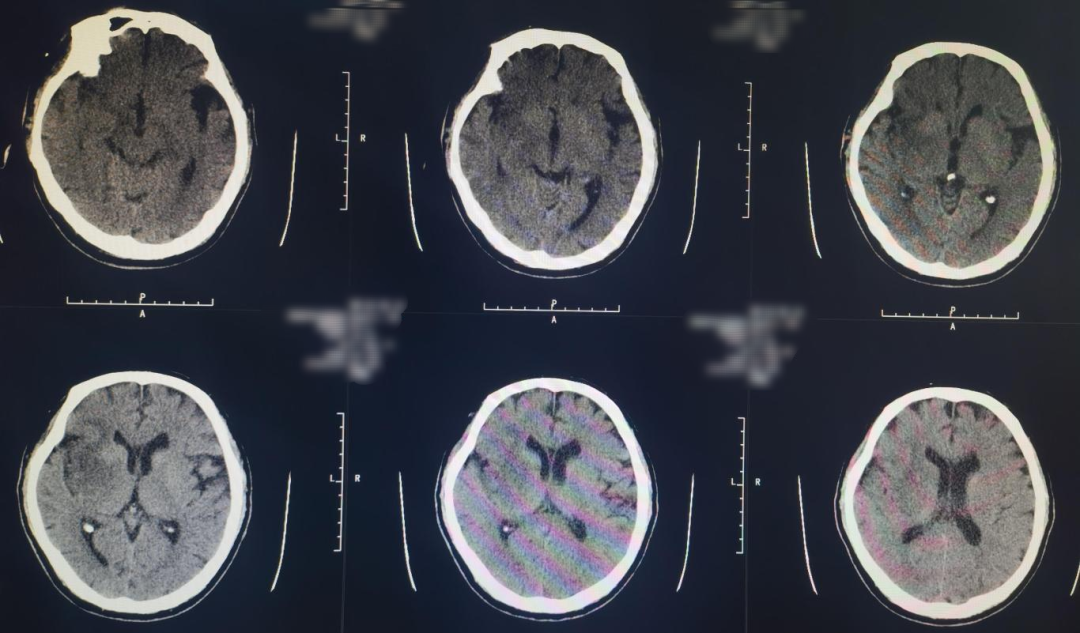
10-day postoperative follow-up cranial CT showed infarction in the right cerebral hemisphere.
Physical examination: patient alert and responsive, speech less fluent, left limb muscle strength grade 3, right limb strength normal. NIHSS score: 6.
Surgeon Information
Shengshan Li, Gaomi Hospital of Traditional Chinese Medicine