

A Case of Aspiration Thrombectomy for Left Middle Cerebral Artery Occlusion
Date:2025-07-29Category:Case ReportsViews:1104
Zenith devices used in this case:

Patient Information
- Male, 54 years old
- Sudden onset of impaired movement in the right limb accompanied by speech loss for approximately 2 hours.
- Muscle strength: Right upper limb – Grade 1, Right lower limb – Grade 3, Left limbs – Normal
- NIHSS score: 12 points
- MRS score: 4 points
Preoperative Angiography
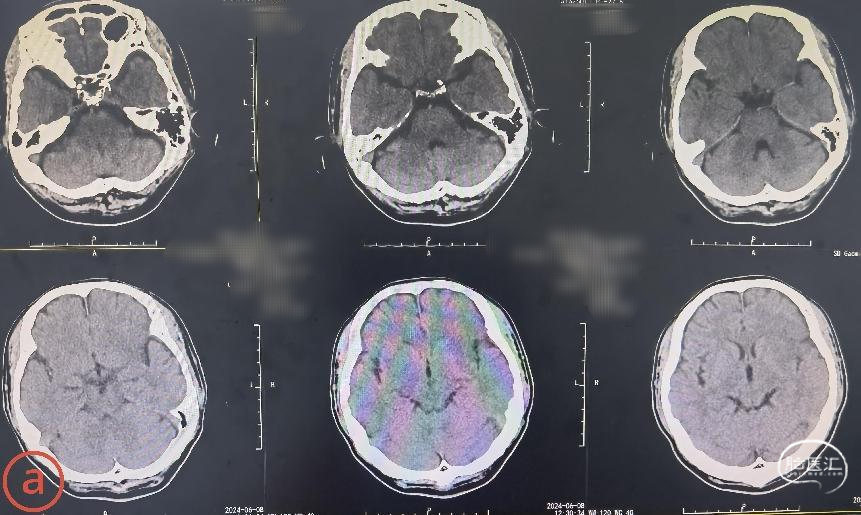
Preoperative cranial CT: High-density sign in the left middle cerebral artery, suggestive of thrombus formation and left cerebral infarction.
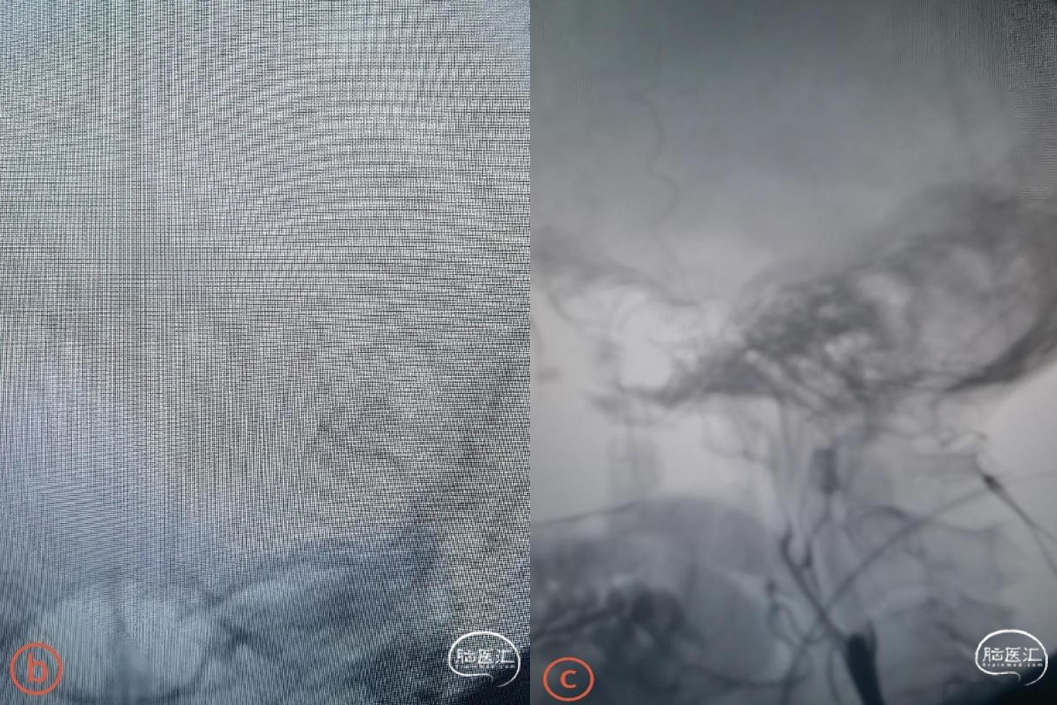
Left internal carotid artery angiography: Occlusion of the left internal carotid artery with no collateral circulation in the left anterior cerebral artery or left middle cerebral artery, and no compensatory blood supply. The left internal carotid artery was identified as the culprit vessel.
Devices
- 6F Zenith Aspiration Catheter
- MPA 8F Guiding Catheter
- 014in*200cm、0.014in*300cm Micro Guidewire
- 5mm*15mm、4.0*30mm Balloon Catheter
- Microcatheter
- 0mm Embolic Protection System
- 9*40mm Carotid Stent
Procedure
A microguide wire and microcatheter successfully navigated through the occluded segment at the origin of the right internal carotid artery. Contrast injection through the microcatheter confirmed entry into the true lumen of the internal carotid artery, while also revealing a lack of opacification in the left middle cerebral artery.

A small balloon was used to dilate the proximal right internal carotid artery to facilitate advancement of the aspiration catheter. The aspiration catheter, guided coaxially with a guiding catheter and assisted by the microwire and microcatheter, was further advanced. Angiography through the microcatheter confirmed placement within the true lumen of the left middle cerebral artery. The aspiration catheter was positioned at the occlusion site, and thrombus aspiration was performed, restoring blood flow.
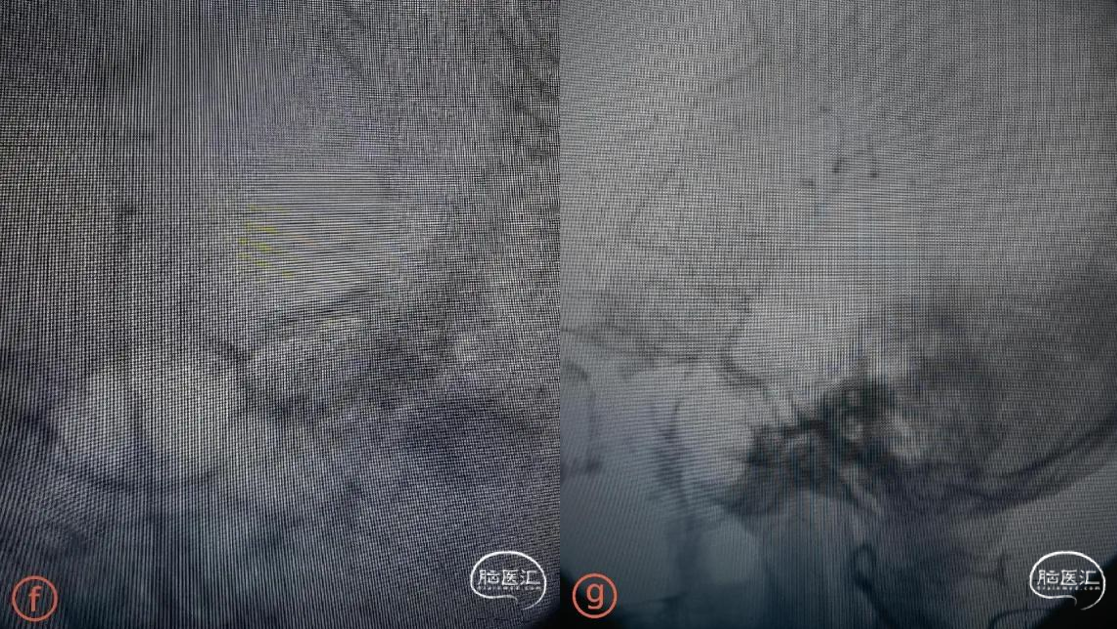
Embolic protection system was carefully navigated along the microwire past the stenotic segment into the petrous portion of the left internal carotid artery. A peripheral balloon dilation catheter was advanced along the protection system microwire to dilate the stenotic segment. The balloon catheter was withdrawn, and a Wallstent stent was delivered and deployed at the stenotic site. Post-deployment angiography showed good stent apposition, with residual stenosis of approximately 20%, improved anterograde blood flow, and restoration of intracranial circulation (TICI Grade 3).

Postoperative Angiography
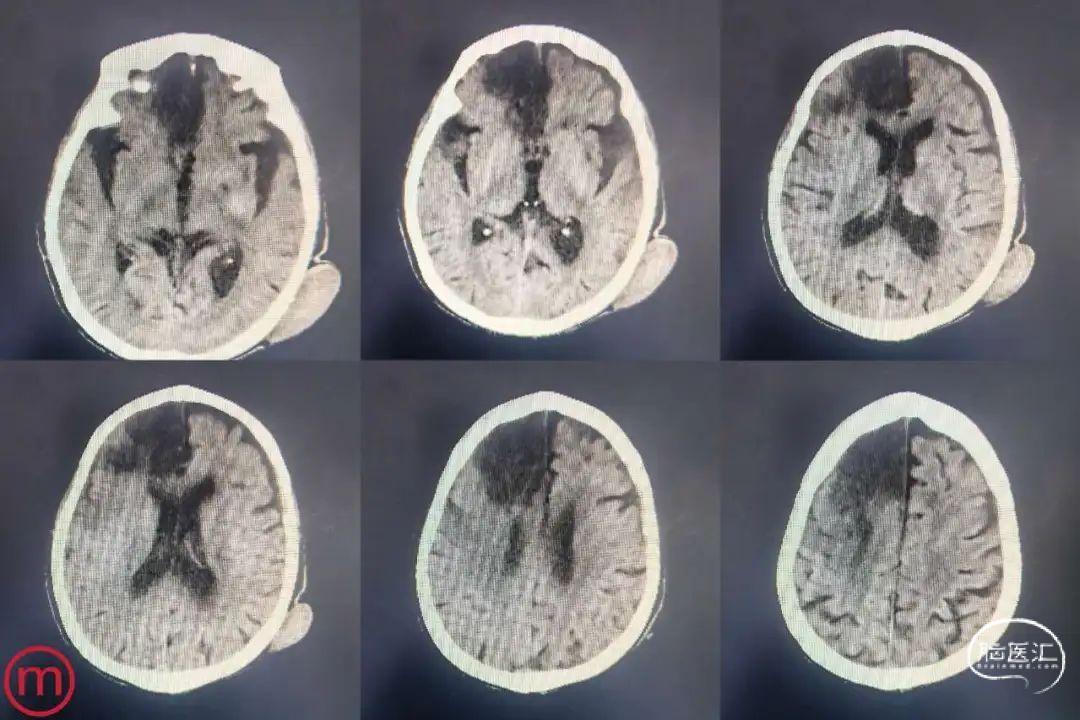
Immediate postoperative cranial CT showed no secondary hemorrhage.
Six hours postoperatively: Muscle strength – Left upper limb: Grade 1, Left lower limb: Grade 3+, Right limbs: Normal. NIHSS score: 8 points
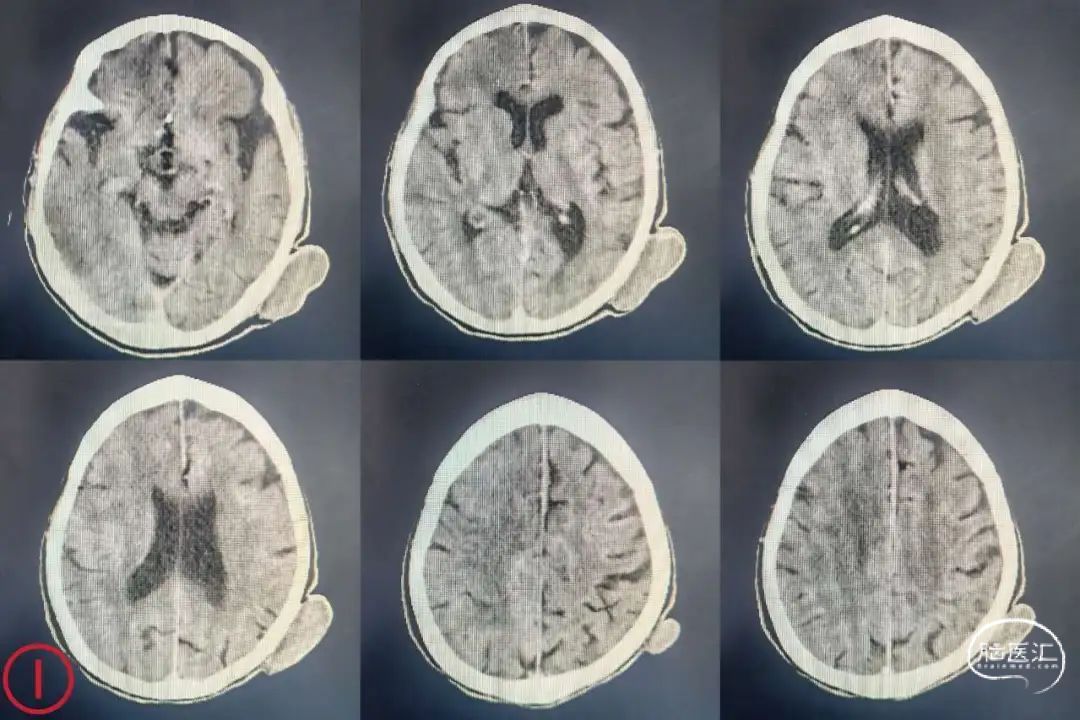
Ten days postoperatively follow-up cranial CT showed a right cerebral infarction.
Physical examination: Left upper limb – Grade 1 muscle strength, Left lower limb – Grade 3+, Right limbs – Normal. NIHSS score: 6 points
Surgeon Information
Shengshan Li, Gaomi Hospital of Traditional Chinese Medicine